
The Genetics of Thrombophilia
Written by: Elizabeth Varga, M.S.
Thrombophilia is a medical term used to describe the condition where the blood has an increased tendency to clot. There are many reasons why the blood can have this increased tendency.
Thrombophilia is usually categorized into two types–acquired and inherited. In acquired thrombophilia the abnormal clotting is usually related to a specific cause, such as prolonged periods of bed rest after surgery, trauma to the leg, or having cancer. People with inherited thrombophilia tend to form clots due to a genetic predisposition inherited from their parents. People with inherited thrombophilia may have a family history of relatives with abnormal or excessive blood clotting. This brochure will explain how genes play a role in blood clotting and are related to inherited thrombophilia.
Blood clotting (coagulation)
Blood clotting is the body’s natural defense against bleeding. A clot, or “thrombus”, develops whenever there is damage to a blood vessel (arteries and veins). Clots are formed through a series of chemical reactions between special blood cells (platelets) and proteins in the blood (clotting factors). The platelets and factors work together to regulate the clotting process; in other words, they start and stop clotting as the body needs it. If the process does not work correctly, a clot can form in the blood vessels, blocking blood flow to the surrounding tissues. When this happens the clot is called a thrombosis.
Thrombophilia and the clotting process
In order for the clotting process to work, clotting factor proteins need to be present in the right amounts and work correctly. People who have inherited thrombophilia may not make the right amount of a specific clotting factor, or the factor may be abnormal in some way. These people tend to develop a thrombosis more easily or frequently than people who do not have inherited thrombophilia.
Proteins and blood clotting
Proteins are large molecules that give the body structure, help it to function, and regulate the way it works. There are many proteins in the body and each protein has a unique function. The process of blood clotting is an example of proteins working together. Blood cells, platelets and clotting factors are all made up of proteins. If there is a problem with these proteins, this can lead to problems with blood clotting.
Genetics, proteins, and blood clotting
To understand how genetics influences blood clotting, it is important to understand how proteins are made:
Blood clotting proteins, like all proteins, are made by linking together a chain of chemicals called amino acids. The order of the amino acids in the chain make up a specific protein; this order is determined by our genes, which are inherited by us from our parents. Genes consist of DNA, which contains our genetic code.
DNA is a molecule shaped like a twisted ladder, and is made up of trillions of chemical bases. These chemical bases are organized in sets of three and “read” by the body much like a sentence. A, T, G, and C are the “letters” of the DNA “alphabet”, or code; they stand for the chemicals adenine, thymine, guanine, and cytosine, respectively, that make up the chemical bases of DNA. Each three-letter code represents a specific amino acid. Just as your brain is able to assign meaning to words, your body is able to assign specific amino acids to each three-letter DNA code.
A segment of DNA code looks like this:
AGCCGTACGGTTCAACCG
The body reads it as:
ACG-CGG-ACG-GTT-CAA-CCC
Based on this, the amino acids are assigned creating a chain of amino acids that makes a protein. Problems arise if there is a spelling error (mutation) in the DNA code. Mutations in the DNA code may result in an incorrect amino acid being assigned.
DNA with a mutation causes a change in the amino acid assigned at a certain position:
ACG-CAG-ACG-GTT-CAA-CGG
If this occurs, the protein that is being made is altered. This alteration could cause the protein to be a different shape or could cause the body to make too much protein, thus the function of the protein will be different.
Inherited thrombophilia
- Inherited thrombophilia occurs when an inherited DNA mutation results in the body producing
- too much or too little of a blood clotting protein
- a blood clotting protein that does not function correctly
While there are a number of mutations that can cause inherited thrombophilia, the most common DNA mutations are named factor V Leiden and prothrombin G20210A. Understanding how these two mutations occur can be applied to the other mutations that result in inherited thrombophilia.
Factor V (five) Leiden
All individuals make a protein called factor V that helps blood clot. However, there are certain individuals who have a DNA mutation in the gene used to make the factor V protein. These individuals are said to have the “factor V Leiden” mutation. The mutation was named after a city called Leiden, where research on the first family found to have the mutation was performed. Individuals with the factor V Leiden mutation have inherited thrombophilia.
Factor V Leiden and the tendency to develop blood clots
Normally the factor V protein is produced to help the blood clot, and is produced in greater amounts after a blood vessel is damaged.
The amount of factor V protein produced is controlled by other proteins, including protein C and protein S. Protein C and protein S combine to help break up factor V, thus preventing it from being reused and clotting the blood.
When a person has factor V Leiden, the mutation causes the protein to be abnormally shaped. This abnormal shape prevents it from being broken down properly by proteins C and S. Since the factor V protein is not broken down, it is left in the blood for a longer period of time and increases the tendency for clotting.
Testing for factor V Leiden
- Factor V Leiden testing is done by taking a blood sample, and there are two types of tests that can be done to determine whether a person has factor V Leiden.
- In some cases, a sample may be tested to see if the blood is resistant to activated protein C (one of the proteins that helps control factor V).
- If the blood is resistant to activated protein C, there is a 90-95% likelihood that the person has a mutation in the factor V gene.
- A genetic test is usually done to confirm the activated protein C blood test. Sometimes, the genetic test is ordered first, without ever doing the activate protein C testing. In this case, the DNA is isolated from blood cells and the factor V gene is examined to see if there is a mutation in the DNA code. If a mutation is found, then the person has factor V Leiden.
Prevalence of factor V Leiden
It is estimated that about 5% (1 out of 20) of Caucasians (white people) have factor V Leiden, and it is more common in individuals of European ancestry. In the United States, approximately 1-2% (1 in 100 to 1 in 50) of African Americans, Hispanic Americans and Native Americans also have the mutation. Factor V Leiden is rare in Asians.
Prothrombin G20210A mutation
All individuals make the prothrombin (also called factor two) protein that helps blood clot. However, there are certain individuals who have a DNA mutation in the gene used to make prothrombin (also called prothrombin G20210A or the factor II (two) mutation). They are said to have an inherited thrombophilia called prothrombin G20210A. When this occurs, they make too much of the prothrombin protein.
Prothrombin G20210A and the tendency to develop blood clots
- Normally, the prothrombin protein is produced to help the blood clot, and is produced in greater amounts after a blood vessel is damaged.
- People who have a mutation in the prothrombin gene produce more prothrombin protein than is normal. Since there is more of the prothrombin protein in the blood, this increases the tendency for clotting.
Testing for prothrombin G20210A
Prothrombin testing is done by taking a blood sample, and using a genetic test to look at the prothrombin gene.
- The DNA is isolated from blood cells and the prothrombin gene is examined to see if there is a mutation in the DNA code. If a gene change is found (the 20210st letter is changed from a G to an A), then the person has a prothrombin (or factor II) mutation.
Prevalence of prothrombin G20210A
A change in the prothrombin gene is present in 2-4% (or 1 in 50 to 1 in 25) of Caucasians, and is more common in individuals of European ancestry. In the United States, approximately 0.4% (about 1 in 250) of African Americans also have the mutation. Prothrombin G20210A mutation is rare in other groups.
Inheritance of factor V Leiden and prothrombin G20210A
Genetic mutations are passed from generation to generation, because we receive our DNA from our parents. Our genetic information is inherited in pairs. Every gene has two copies; one comes from our mother and one from our father. Different conditions can be inherited in different ways; thrombophilia is considered a dominant trait. That means a person with inherited thrombophilia only has to have a mutation in one of his/her two gene copies to have the condition. This is also called dominant inheritance.
If a person inherits only one copy of the gene mutation, they are said to be heterozygous (“hetero” means different, “zygous” means bodies). If both copies of a person’s gene have a mutation, they are said to be homozygous (“homo” means same, “zygous” means bodies).
If a person is homozygous (that is, he or she inherits a mutation in both copies of their gene, one from each parent) they are at a greater risk to develop a blood clot than an individual who is heterozygous.
An individual can also have a greater risk to develop a blood clot if they inherit a mutation in more than one of the genes that lead to thrombophilia. For example, a person has a greater risk to develop a blood clot if they have both factor V Leiden and prothrombin G20210A.
Chance to inherit thrombophilia
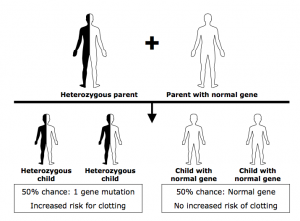
Every individual inherits two copies of each gene. One copy is inherited from their mother, the other copy from their father. To predict the risk to a child, a few factors must be considered.
The first is whether or not you are heterozygous (only one of your two gene copies contains a mutation) or homozygous (both copies of your two genes contain a mutation). A genetic test can tell you whether you are heterozygous or homozygous.
The first is whether or not you are heterozygous for the gene mutation, there is a 50:50 (or one half) chance that your child will inherit the gene mutation, because there is an equal chance of passing on the gene copy with the mutation OR the gene copy without the mutation. The gene copy your child inherits is due to chance, and there is nothing an individual can do to alter this chance. (See diagram below.)
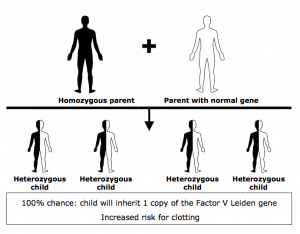
If you are homozygous for the gene mutation, your child will inherit the mutation. Since you do not have a copy of the gene without a mutation, it is impossible to pass on a gene without a mutation to your child.
Another consideration is whether the child’s other parent carries a gene mutation that leads to thrombophilia. This would also influence your child’s chances of inheriting thrombophilia.
Genetic counselors are medical professionals who can help interpret genetic concepts. If you are interested in learning more about genetic risks, you can consult with a genetic counselor, or a healthcare professional who has specialized training in genetics. To locate a genetic counselor in your area, you may contact the National Society of Genetic Counselors at http://www.nsgc.org.
Genetic testing of family members
There are many issues surrounding the decision to pursue genetic testing. It is important to consider how genetic information will be used in medical management before having any testing done. It is recommended that these issues be discussed with a knowledgeable healthcare provider. You may also wish to see the NBCA brochure entitled Family Testing for Blood Clotting Disorders for more information.
Disclaimer
The National Blood Clot Alliance (NBCA) and its Medical and Scientific Advisory Board (MASAB) do not endorse or recommend any commercial products, processes, or services. The views and opinions of authors expressed on the NBCA or MASAB websites or in NBCA or MASAB written materials do not necessarily state or reflect those of NBCA or MASAB, and they may not be used for advertising or product endorsement purposes.
It is not the intention of NBCA or MASAB to provide specific medical advice, but rather to provide users with information to better understand their health and their diagnosed disorders. Specific medical advice will not be provided and both NBCA and MASAB urge you to consult with a qualified physician for diagnosis and for answers to your personal questions.
Current News

Follow us on Instagram

